

This article was written by Assoc. Prof. Dr. Burak Sercan Erçin and is based on clinical experience. A specialist in Plastic, Reconstructive and Aesthetic Surgery; prepared in accordance with current medical literature and personal surgical data. A consultation is recommended before making any medical decisions.

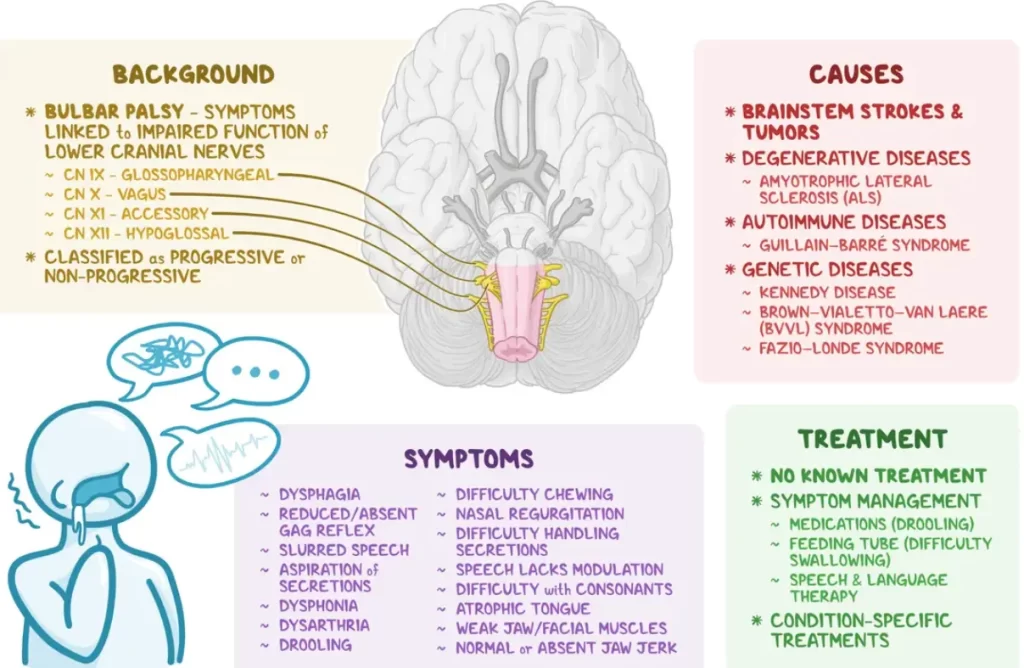
Bulbar facial palsy is a neurological condition that affects the nerves in the brainstem (specifically the medulla oblongata) which control the muscles used for speaking, chewing, swallowing, and some facial movements. The term “bulbar” comes from the bulb-like shape of this part of the brainstem. Damage to these nerves causes weakness in the tongue, throat, and facial muscles.
Bulbar palsy can be progressive (worsening over time, usually due to a disease like ALS) or non-progressive (stable, often due to a one-time injury like a stroke). It’s important for patients and caregivers to recognize that the early symptoms are often related to speech and swallowing. Treatment focuses on managing these symptoms to improve comfort and safety. Many people with progressive bulbar palsy live only a few years after diagnosis, so understanding the condition and planning supportive care is essential.
The brainstem (shown here in a midline diagram) includes the medulla oblongata (“bulbar” region) at its base. The medulla contains the nerve nuclei for cranial nerves that control speech and swallowing muscles. Bulbar palsy refers to weakness in these medulla-controlled muscles.
- Affects speech and swallowing: Bulbar palsy weakens the muscles that move the tongue, lips, and throat. This leads to slurred or nasal speech and difficulty swallowing, which are often the first signs to appear.
- Distinct from ALS: Progressive bulbar palsy is considered a type of motor neuron disease similar to ALS (Lou Gehrig’s disease). However, “bulbar palsy” itself describes the pattern of symptoms (weakness of bulbar muscles) and can be caused by several different conditions.
- No cure for progressive cases: Unfortunately, if bulbar palsy is due to a degenerative disease like ALS, there is no cure. Treatment is supportive (feeding tubes, speech therapy, medications for symptoms) to help maintain comfort and function as long as possible.
- Rare condition: Bulbar palsy is uncommon. Only a small fraction of people have the bulbar form of ALS (roughly one-quarter of ALS cases start in the bulbar muscles). Overall, the incidence of ALS is about 1–2 cases per 100,000 people per year, so bulbar-onset cases are relatively rare among the general population.
Disease Prevalence
Bulbar palsy itself is not a common diagnosis. It is most often seen in connection with serious neurological diseases. Progressive bulbar palsy is typically part of motor neuron disease; for example, about 20–30% of ALS cases begin with bulbar symptoms. Because ALS is rare, bulbar palsy from ALS is even rarer. Non-progressive bulbar palsy (from causes like stroke or tumor) is also uncommon. In general terms, only a few people per 100,000 develop bulbar-type symptoms each year.
How rare is progressive bulbar palsy?
Progressive bulbar palsy is a rare form of motor neuron disease. Remember that ALS (both bulbar- and limb-onset) is itself rare (about 2 out of 100,000 people each year). Of those, only about one in four will have their first symptoms in the bulbar muscles. In other words, bulbar-onset ALS might occur in roughly 0.5 per 100,000 people per year. These numbers mean that most doctors and patients will not encounter many cases in their careers.
Cure
Bulbar palsy cure
Currently there is no cure for progressive bulbar palsy or bulbar-onset ALS. Medical science has not found a way to reverse the underlying nerve damage. Instead, treatments aim to slow progression and ease symptoms:
- Medications for ALS: Drugs such as riluzole and edaravone are approved for ALS and may slightly slow nerve damage, but they do not stop the disease or cure bulbar palsy. They might extend survival by a few months in some cases.
- Supportive therapies: Because no treatment can repair the damaged nerves, focus is on symptom relief. For example, feeding tubes can ensure nutrition if swallowing fails, and speech therapy or communication devices help with talking.
- Manage complications: Therapies like physical therapy can help maintain posture and mobility for as long as possible. Medications can control drooling or spasticity. Palliative care and hospice support are important parts of care, especially in advanced stages.
If bulbar palsy is due to a treatable cause (like a stroke or tumor), then addressing that cause (clot-busting drugs, surgery, or radiation) can prevent further damage. In those cases the condition is not really “cured” but may become stable or even improve somewhat. For the progressive forms (e.g. ALS), even the best medical treatment cannot restore lost function.
Causes
What causes bulbar palsy?
Bulbar palsy results from any damage to the lower motor neurons (nerve cells) that control the bulbar muscles. These nerves (cranial nerves IX, X, XI, and XII) emerge from the medulla in the brainstem. Causes fall into two broad categories:
- Degenerative diseases: The most well-known is Amyotrophic Lateral Sclerosis (ALS). In the ALS variant called Progressive Bulbar Palsy, the nerve cells in the medulla slowly degenerate. Over time, this kills the nerves and leads to worsening muscle weakness.
- Structural lesions: Things that physically injure the brainstem can cause bulbar palsy too. For example, a brainstem stroke (bleeding or clot in the medulla) can suddenly damage those nerves. A tumor or infection in the medulla can also do the same. These are non-progressive causes (the damage happens once and then stays fixed).
- Autoimmune or inflammatory diseases: Sometimes the immune system attacks nerves. Conditions like Guillain–Barré syndrome (a nerve inflammation) or multiple sclerosis (which usually affects upper nerves but can involve the brainstem) can lead to bulbar symptoms. Neurosyphilis or Lyme disease rarely cause isolated bulbar palsy, but they can affect the brainstem.
- Genetic conditions: Kennedy’s disease (a type of X-linked spinal and bulbar muscular atrophy) is a genetic cause of bulbar weakness. People (usually men) with this condition gradually develop limb and bulbar muscle problems.
- Toxins and infections: Certain toxins like botulism can block nerve signals to those muscles, causing sudden bulbar palsy. Early poliovirus infection (or its rare late effects) can affect the bulbar nerves.
- Other causes: Head injuries that impact the medulla, or nutritional deficiencies, are much less common causes. Even myasthenia gravis – a disease of the neuromuscular junction – can initially look like bulbar palsy (though it’s technically not the same mechanism).
Because bulbar palsy symptoms can arise from many different problems, doctors will usually do tests to find the cause. This includes brain MRI/CT scans to look for strokes or tumors, blood tests for infections or autoimmune markers, and electrical studies (EMG) to look for nerve degeneration. Identifying the cause is important because some causes (like stroke or infection) are treatable.
Early Signs
Bulbar palsy initial symptoms
Early symptoms of bulbar palsy are often subtle and easy to overlook, because they involve basic functions everyone does every day. Patients may notice:
- Speech changes: The voice may become hoarse, nasal, or slurred. Words might come out softly or slowly. You might notice that people begin to ask you to repeat yourself more often. Sometimes the change is described as “mumbling.”
- Swallowing difficulty: There may be trouble swallowing pills or certain foods. Patients can cough or choke when eating or drinking. You might notice food “sticking” in the throat or nasal regurgitation (food coming back up into the nose).
- Drooling: Because the tongue and throat muscles are weak, saliva may pool in the mouth and dribble out, especially when speaking or lying down. Patients often feel they can’t swallow normally.
- Weak tongue: Activities like sticking out the tongue or pushing it against a tongue depressor may reveal weakness. The tongue might drift to one side or exhibit twitching (fasciculations). Even in early stages, the tongue can feel heavy or clumsy.
- Facial and jaw weakness: The jaw muscles might tire when chewing, leading to difficulty eating tough foods. The lips or cheeks may seem floppy on one side. Sometimes the angle of the mouth droops slightly.
- Voice changes: The term dysphonia means difficulty in voice; early on it may seem just hoarse or raspy, sometimes with a “whispery” quality. This often gets worse over time.
These symptoms generally start on one side or mild on both sides and progressively worsen. Because they affect everyday tasks, even slight speech or swallowing changes should prompt medical attention in a timely manner. Note that bulbar palsy does not affect your intelligence or emotions – it only affects the muscle control. At first, patients usually still understand and know exactly what they want to say.
Age
Bulbar palsy age
The age of onset for bulbar palsy depends on its cause:
- Degenerative cases (ALS/PBP): These typically occur in middle to late adulthood. Most people develop symptoms after age 40, often in their 50s or 60s. There is no exact cutoff – bulbar-onset ALS has been reported in people as young as 30s and as old as 80s, but on average it is a mid-to-late adult condition.
- Non-progressive causes: Strokes or brainstem tumors can happen at any adult age, but are more common in older adults (stroke risk increases with age). A stroke in the medulla is most likely in someone who already has cardiovascular risk factors like high blood pressure or diabetes.
- Genetic causes: Kennedy’s disease (an inherited cause of bulbar weakness) typically appears in men in their 20s–40s, which is younger than most ALS cases. Fazio-Londe syndrome (a rare juvenile bulbar palsy) can occur in children and teens, but this is extremely rare and has different features.
- Children: True bulbar palsy is very rare in children. If an infant or child has bulbar-type symptoms (feeding problems, weak cry, drooling), doctors investigate congenital or genetic neuromuscular diseases.
In summary, bulbar palsy usually appears in adulthood. Progressive bulbar palsy (ALS type) is mainly a disease of later middle age. If a child or very young adult shows bulbar symptoms, alternative diagnoses (like congenital brainstem problems or metabolic diseases) are considered first.
Pseudobulbar vs Bulbar Palsy
It’s important to distinguish bulbar palsy from pseudobulbar palsy, since they sound similar but have different causes and some different features:
Cause: Bulbar palsy comes from damage to the lower motor neurons in the brainstem or the cranial nerves themselves. Pseudobulbar palsy comes from damage to the upper motor neurons (the brain’s corticobulbar tracts) that control those same muscles. In practice, pseudobulbar palsy is often seen after two-sided (bilateral) strokes, multiple sclerosis, or advanced motor neuron disease, whereas bulbar palsy is from direct brainstem injury or a lower neuron disease.
Speech and swallowing: Both can cause slurred speech (dysarthria) and swallowing trouble (dysphagia). However, the quality differs. In bulbar palsy, the speech is usually weak, breathy, or nasal because the muscles are floppy. In pseudobulbar palsy, speech is more strained or tight (patients often sound forced or spastic).
Facial movements and reflexes: Bulbar palsy often causes muscle wasting (atrophy) and fasciculations (small twitches) in the tongue or face. The jaw jerk reflex tends to be reduced or normal. In contrast, pseudobulbar palsy causes spasticity: the facial muscles are stiff, with an exaggerated jaw jerk and gag reflex. The lips may press together tightly, making emotional expression difficult.
Emotional control: One key difference is emotional expression. Pseudobulbar palsy often leads to uncontrollable laughing or crying (called pseudobulbar affect) that is inconsistent with how the person actually feels. For example, a patient might burst into tears or laughter out of proportion to their mood. In true bulbar palsy, emotions are generally unaffected – patients do not have these involuntary emotional outbursts. Their affect (emotional tone) is appropriate.
Eyes and eyebrows: With pseudobulbar palsy, there may be excessive blinking and a wrinkled brow with exaggerated facial movements. Bulbar palsy may weaken facial expressions more on one side, and the eyebrows may droop slightly.
To sum up: Bulbar palsy = LMN (lower motor neuron) damage – floppy face and tongue, weakness, atrophy, drooling, no involuntary emotions. Pseudobulbar palsy = UMN (upper motor neuron) damage – spastic, stiff speech, exaggerated reflexes, and episodes of uncontrollable laughter/crying. Despite the differences, both conditions need evaluation by a doctor because the treatments and underlying causes differ greatly.
Bulbar Palsy Symptoms
Bulbar palsy affects many functions of the mouth, throat, and lower face. The symptoms can be grouped into problems with speech, swallowing, and secretions:
- Speech problems (dysarthria): Speech may become slow, slurred, or nasal. Patients often describe it as sounding “muffled” or “like talking underwater.” Initially it may be hard to notice, but gradually words become less clear. Some have a “monotone” voice because they can’t change volume well. As it worsens, patients may be unable to speak clearly at all.
- Swallowing difficulties (dysphagia): Chewing and moving food around with the tongue become hard. People may cough or choke on food or liquids. There is a risk of aspiration (food or saliva entering the airway) which can cause pneumonia. Patients often take a long time to eat or may avoid certain foods (like breads or meats) because they are hard to swallow.
- Drooling and secretions: Weak throat muscles make it hard to clear saliva. As a result, there is often excessive drooling (sialorrhea). Patients may feel as if their mouth is full of saliva that they can’t swallow. Drooling can be constant and embarrassing, and it increases the risk of choking.
- Weak tongue: The tongue may appear thin (atrophic) and may tremble or twitch when trying to move it. Patients may notice the tongue deviating to one side when sticking it out. Because the tongue is so important for speech and swallowing, even mild tongue weakness greatly affects these functions.
- Facial weakness: The face may look expressionless or droopy. Smiling, puckering lips, or closing eyes tightly can be difficult. The jaw muscles weaken too, so biting down or chewing is hard. Some patients find their jaw “gives out” or feels heavy.
- Voice changes (dysphonia): The voice may sound weak, hoarse, or breathy. Sometimes it becomes very quiet or even whispers. A nasal quality is common (as if talking with a stuffy nose) because the soft palate doesn’t close properly.
- Gag reflex loss: Doctors may note a reduced or absent gag reflex. Patients themselves might feel like something is “off” when they swallow because the back of the throat isn’t responding normally.
- Breathing issues: In very advanced bulbar palsy, breathing can become difficult. Since the muscles of the upper airway are weak, patients can have noisy breathing or stridor. Sleep breathing problems (like snoring or pauses) can occur.
Bulbar palsy symptoms typically affect both sides (bilateral), but one side may lag behind the other. Over weeks to months, the above symptoms tend to progress. Early on you may see only slurred words and drooling; later on, speech becomes nearly impossible and swallowing may require a feeding tube. Throughout all this, cognition and sensation are spared – thinking and feeling are normal, so patients are fully aware of what is happening to their bodies.
Bulbar Palsy Treatment Options
Since there is no cure for progressive bulbar palsy, treatment is centered on maximizing quality of life and safety. The approach includes medical therapies, supportive devices, and therapy services:
Disease-modifying drugs: For ALS-related bulbar palsy, doctors may prescribe riluzole or edaravone. These medications aim to slow nerve injury. Riluzole can extend survival by a few months on average; it is most effective early in the disease. Edaravone is given by IV and may also slow progression in some patients. These drugs are not cures, but they are standard parts of ALS care.
Swallowing and nutrition support: A swallow specialist or speech therapist can teach techniques to make swallowing safer (like chin tucks or special head positions). If swallowing becomes very unsafe, a feeding tube (gastrostomy tube) is placed. This allows nutrients and medicines to be delivered directly to the stomach. Feeding tubes greatly reduce choking risk and help maintain weight. Some people with bulbar palsy live with a feeding tube for months or years.
Speech support: Speech therapy can help maintain any existing speaking ability. Therapists teach communication techniques (like pacing and over-articulation). When speech becomes too difficult, alternative communication devices are used. These range from simple picture boards to high-tech voice synthesizers controlled by eye movement or minimal muscle contractions. The goal is to preserve the patient’s ability to express needs and feelings even if spoken words fail.
Respiratory support: Breathing can weaken as bulbar palsy advances. Non-invasive ventilation (e.g. BiPAP machines worn at night) can assist breathing during sleep and later even during daytime. This helps with fatigue and breathlessness. In some cases, a tracheostomy (breathing tube through the neck) and full ventilator support may be considered, although not all patients choose this due to the advanced nature of the illness.
Medication for symptoms: Drooling can be managed with medications that dry up saliva (anticholinergic drugs like glycopyrrolate or scopolamine). Botox injections into the salivary glands are another option. If spasticity (rare in pure bulbar palsy) or stiffness occurs, muscle relaxants like baclofen may help. Those with emotional lability (pseudobulbar affect) can sometimes be helped with antidepressants or a drug called dextromethorphan-quinidine (Nuedexta).
Physical and occupational therapy: Keeping the neck and shoulder muscles strong can help with posture and comfort. Therapists may suggest neck braces or swallowing exercises early on. Assistive devices (special utensils, adaptive seating) are prescribed to make eating and daily tasks easier as weakness progresses.
Treatment of underlying cause: If bulbar palsy is not from ALS but from another treatable condition, therapy focuses on that. For example, if due to a stroke, rehabilitation and possibly medications to prevent further strokes are given. If a tumor is found, surgery or radiation might relieve symptoms. In autoimmune cases, immunosuppressive therapies (like steroids or IVIG for Guillain–Barré) are used.
Palliative care and planning: Early involvement of palliative care specialists improves comfort and planning. This team can help manage symptoms (pain, anxiety, secretions) and discuss goals of care. Advanced directives and hospice care planning should be addressed early, since progressive bulbar palsy declines rapidly.
In all cases, treatment is customized to the patient’s needs and wishes. The focus is on preserving communication, nutrition, and breathing as long as possible, and on keeping the patient comfortable. Family education and support are also crucial, as caregivers often need to assist with feeding, communication, and personal care.

Don’t miss out on Dr. Burak’s Expertise
Contact him now !
Bulbar Palsy Life Expectancy
Progressive bulbar palsy carries a poor prognosis. By the time bulbar symptoms appear, many of the essential breathing and swallowing muscles have been affected. On average, patients with ALS who start with bulbar symptoms survive about 1 to 3 years after symptom onset. In some studies, the range is quoted as roughly 6 months to 3 years. Survival time tends to be shorter than in classic limb-onset ALS. Some factors influence life expectancy: rapid weight loss, respiratory weakness, and development of limb weakness soon after bulbar onset generally predict a shorter survival.
Important distinctions:
- Progressive bulbar palsy (ALS-related): Life expectancy is often under 3 years. The disease is fatal because it eventually affects breathing. Many patients may spend their final days in hospital or hospice, often due to pneumonia or respiratory failure.
- Bulbar-onset ALS: This is essentially the same as progressive bulbar palsy. Studies show bulbar-onset ALS has a faster course than limb-onset. Patients often lose the ability to breathe on their own within a year or two of diagnosis.
- Non-progressive bulbar palsy: If the cause is a one-time event (like a stroke or tumor that has been treated), then bulbar symptoms may stabilize. In that case, bulbar palsy itself does not shorten lifespan by itself. For example, a person might recover partially from a brainstem stroke and live a normal life expectancy aside from disabilities. Here the life expectancy depends on the underlying cause (and general health), not on “bulbar palsy” per se.
In summary, progressive bulbar palsy due to ALS is typically fatal within a few years, and patients are usually advised to plan for end-of-life care. In contrast, bulbar palsy from a stable injury does not inevitably lead to death, though it may cause disability.
Final Stages of Bulbar Palsy
In the final stage of progressive bulbar palsy, patients lose almost all voluntary control of the bulbar and respiratory muscles. Key features of this phase include:
- Severe swallowing impairment: The throat muscles can no longer move food or saliva. Patients often rely entirely on a feeding tube if they have not already. Even swallowing saliva becomes impossible. Caregivers must suction the mouth and throat frequently to clear secretions, or patients can choke.
- Communication loss: Speech may be completely lost. Even aided communication devices become difficult to use if the patient is weak or unresponsive. Most communication in this stage is by gestures or eye movements.
- Breathing weakness: The muscles that keep the airway open and inflate the lungs are very weak. Patients often need continuous ventilatory support (BiPAP or a ventilator). Despite this, breathing can become very labored because the brainstem can no longer coordinate breathing and swallowing safely. Many patients experience frequent shortness of breath and fatigue.
- Recurrent pneumonia: Due to chronic aspiration (inhaling saliva or food), pneumonia is very common. Once pneumonia sets in, recovery is unlikely. Infections can become a terminal complication.
- Neurological decline: Aside from bulbar muscles, many patients by this stage have weakness of limb and respiratory muscles too, though some may retain arm/leg strength until very late. The upper motor neurons may also become involved, adding spasticity to the picture (especially if the condition is truly ALS).
- End-of-life considerations: Typically, patients in final stage require around-the-clock care. Comfort measures (pain relief, anxiety control, oxygen therapy) and hospice care become the focus. Life is supported mostly by machines and tubes. Emotional support and palliative sedation may be used to ease suffering from secretions and breathing distress.
In short, the final stage of bulbar palsy is a critical situation. Patients often lose the ability to feed, speak, or breathe without assistance. Healthcare teams emphasize comfort and dignity at this point, as medical efforts to prolong life may become burdensome. Palliative care teams work with families on decisions like whether to continue ventilation or accept hospice.
Non-Progressive Bulbar Palsy Life Expectancy
Non-progressive bulbar palsy means the bulbar weakness comes from a one-time injury (such as a stroke, trauma, or tumor) and does not continue to worsen on its own. In these cases:
- Stabilized condition: After the initial event (for example, a brainstem stroke), the damage to the nerves is done. The remaining bulbar function usually does not deteriorate further. This is very different from ALS, which relentlessly progresses.
- Rehabilitation outcome: Many patients recover partially with therapy. For example, after a stroke some patients regain the ability to eat soft foods and improve speech with rehab. Others may remain severely impaired but stable.
- Life expectancy: There is no specific reduction in lifespan due to the bulbar palsy itself. The prognosis depends on the underlying cause. For instance, someone with a bulbar stroke might have a lifespan similar to other stroke survivors of the same age (adjusted for stroke severity). If a tumor caused it, life expectancy depends on the tumor’s nature and treatment response.
- Exceptions: If the original cause continues (e.g. an untreated infection or an aggressive tumor), then life expectancy is impacted by that cause. But if the cause is fixed (no cancer recurrence, infection resolved), then the patient can live a normal life span, albeit with disabilities.
So, for non-progressive bulbar palsy, think of it as a chronic disability rather than a terminal illness. The focus is on rehabilitation and adaptation, not on managing a fatal illness.
Bulbar Palsy Radiology Findings
Doctors use imaging tests mostly to rule out other conditions that could mimic bulbar palsy, rather than to diagnose bulbar palsy itself. Here’s what to expect:
- Brain MRI/CT: Almost everyone with new bulbar symptoms gets an MRI of the brain and brainstem. This looks for stroke, multiple sclerosis plaques, tumors, or inflammation in the medulla. For most patients with motor neuron disease, the MRI will turn out normal or show only incidental findings. A normal MRI helps support the diagnosis of a neurodegenerative condition like ALS (by excluding other causes).
- “Bright tongue sign”: In rare cases of long-standing ALS with severe tongue weakness, a special MRI finding can appear. This is called the “bright tongue sign,” where the tongue muscles look unusually bright on certain MRI sequences (due to fatty replacement of muscle). It is a subtle clue of chronic bulbar denervation. However, it is not routinely seen in every patient, and it’s more of a research curiosity. Patients should not count on imaging to show bulbar palsy.
- Spinal imaging: Because some conditions (like Guillain–Barré or cervical myelopathy) can cause similar symptoms, doctors might also image the cervical spine. This is to check if nerve roots or upper spinal cord compression are affecting bulbar nerves. Usually, imaging of the neck is unremarkable for bulbar palsy.
- Diagnostic tests: Besides imaging, doctors use electromyography (EMG) and nerve conduction studies to confirm bulbar palsy. EMG can show denervation changes in bulbar muscles and the limbs, which points to ALS. There is no single radiology test that diagnoses ALS or bulbar palsy directly.
In summary, typical imaging in bulbar palsy shows either normal results or findings related to the cause (e.g. a stroke or tumor). Normal imaging with bulbar symptoms usually pushes the diagnosis toward a motor neuron disease, whereas an abnormal brainstem image would suggest a structural cause.
Frequently Asked Questions
- What is the life expectancy of someone with progressive bulbar palsy?
Progressive bulbar palsy (the bulbar-onset form of ALS) significantly shortens life. Most people survive 1–3 years after the first symptoms appear. Some studies report averages around 1–2 years. A small number of patients live longer, but death often occurs due to respiratory failure or pneumonia. - Is bulbar palsy the same as ALS?
Not exactly. “Bulbar palsy” describes a set of symptoms (weak speech/swallowing muscles). Progressive bulbar palsy is essentially the same as ALS that starts in the bulbar region. However, bulbar palsy can also occur from other causes (like stroke or tumor). In practice, if someone has bulbar palsy, doctors will strongly consider ALS, but they must rule out other possibilities. ALS affects both upper and lower motor neurons, while pure bulbar palsy is a lower motor neuron problem. - What are the first signs of bulbar ALS?
The earliest signs are usually subtle speech and swallowing changes. For example, speech might become slightly slurred or raspy, with a nasal tone. The patient may have trouble pronouncing certain sounds or getting words out quickly. Chewing tougher foods may become difficult, or the person may cough more during meals. Drooling may start. Many people notice their voice or swallowing first before limb weakness develops. - Can you recover from bulbar palsy?
It depends on the cause. If bulbar palsy is due to a single event (like a stroke or tumor surgery) and there’s no ongoing disease, some recovery is possible with rehabilitation, and the condition may remain stable. However, if it’s caused by a progressive disease like ALS, there is no recovery of lost function. Therapies may help with symptoms, but true recovery (cure) does not occur in progressive bulbar palsy. - What is the most common cause of bulbar palsy?
In adults, the most frequent single cause of progressive bulbar palsy is ALS (motor neuron degeneration). For non-progressive bulbar palsy, the most common cause is a stroke in the brainstem. In many patient education contexts, “brainstem stroke” and “ALS” are mentioned first. In other words: in a patient who suddenly develops bulbar palsy, doctors often look for stroke or tumor; in a patient with gradually worsening symptoms, ALS is the likely culprit. - What is the life expectancy of a bulbar-onset ALS patient?
Bulbar-onset ALS (where symptoms begin in the bulbar muscles) usually has a shorter survival than limb-onset ALS. On average, life expectancy is around 2 years, with many patients living 1–3 years after onset. Factors like rapid spread to limb muscles, older age, and significant weight loss can make it even shorter.
Each person’s situation is unique, so these answers represent general trends. Medical care should be individualized. It is crucial for patients with bulbar palsy (and their families) to work closely with neurology and palliative care teams to understand their specific prognosis and to plan for care and support.
This content was written by Assoc. Prof. Dr. Burak Sercan Erçin in line with clinical experience and current medical literature. It is intended for general informational purposes only and does not constitute medical advice. A personal consultation with Dr. Erçin is recommended for individual assessment.
Faculty Member · Bahçeşehir University
Graduate of Ege University Faculty of Medicine, Assoc. Prof. Dr. Erçin completed advanced fellowships at Tampa General Hospital (USA) under Dr. Deniz Dayıcıoğlu in breast reconstruction and burn surgery, and at the clinic of Dr. Pedro Cavadas in Valencia, Spain in reconstructive microsurgery. After passing the EBOPRAS examination in 2018, he joined Bahçeşehir University as a faculty member and continues his private practice on Bağdat Avenue, Istanbul, specialising in face, breast and body aesthetics alongside complex reconstructive surgery.







